Using a core components approach
In the Evidence Portal, we have adopted a core components approach to how we collate, use and build evidence. A core components approach organises the research evidence in a way that is meaningful and easily applicable to existing programs and services. It will support us to design and deliver services that are flexible, tailored to local needs and evidence-informed.
What are core components and flexible activities?
Core components are program components that are common across evidence-informed programs. Flexible activities are the different ways that each component can be delivered.
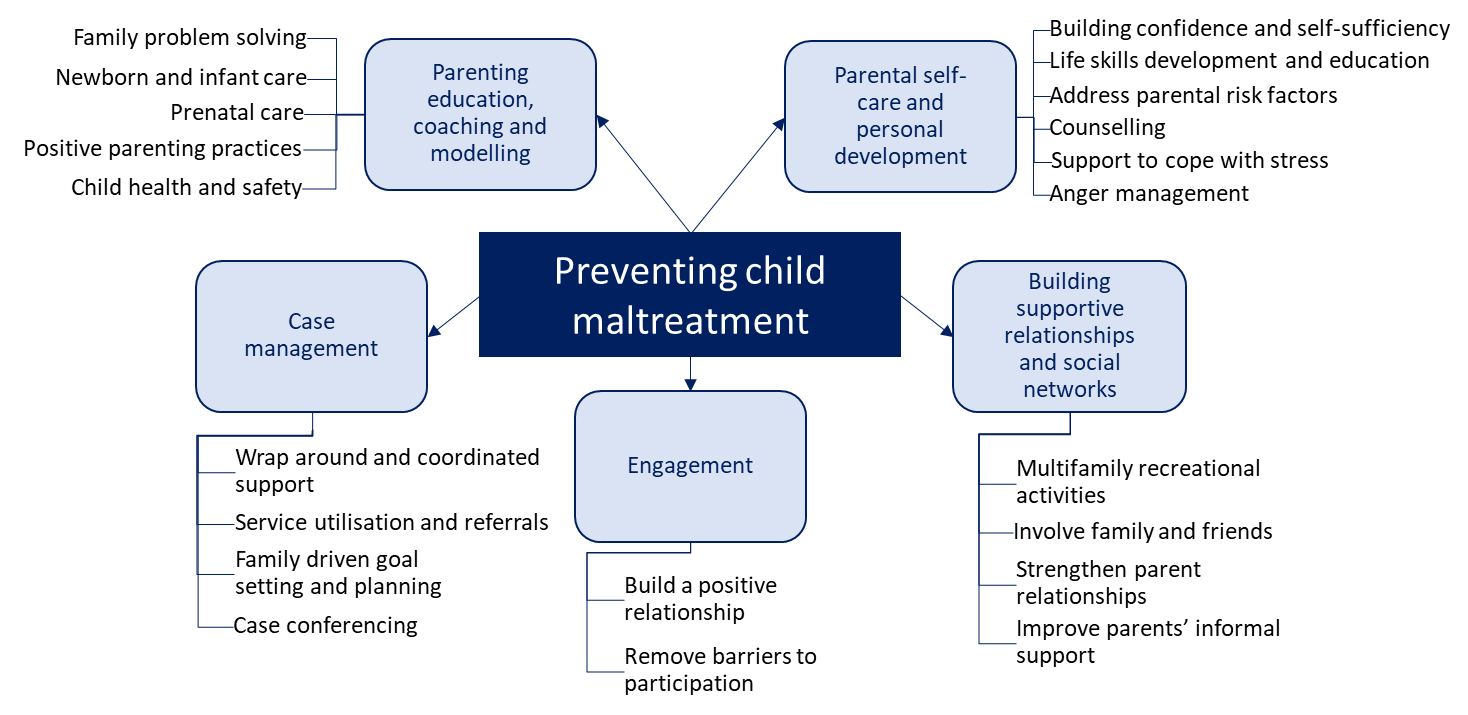
See below for an example of core components to prevent child maltreatment. We conducted an evidence review and identified 5 core components that are common across evidence-informed programs shown to prevent child maltreatment. They make up standardised program components that can be delivered by any program for families at risk of child maltreatment.
Within each component are flexible activities. The flexible activities describe the different ways each core component can be implemented. Practitioners can pick and choose the activities that are most relevant to their clients, the local service delivery context and the resources available to communities.
For example, when working with families at risk of child maltreatment, parental self-care and personal development is important. You could support parents with counselling, anger management, support them to build their confidence and become more self-sufficient.
The support you provide and the services you offer will depend on the specific needs of the clients you work with. You may need to conduct a few of these activities simultaneously, you could focus on one issue at a time, or your client may pick a specific area to address first.
See Preventing Child Maltreatment: What works? for more information.
Core components identified in our evidence reviews
How can core components and flexible activities be used?
You can use the core components and flexible activities in the Evidence Portal to:
- Design a new service: the core components can be used to identify what kind of activities should be provided to your clients and the different ways you can deliver them.
- Adapt an existing service to better meet the needs of your clients: if a particular service you deliver isn’t working, you can use the core components to see if something is missing or what could be done differently.
- Understand how multiple services and supports can work together: the core components can help us identify what other kinds of services and supports we might need to engage with to ensure our clients receive the wrap around support they need.
How are core components and flexible activities identified?
Core components and flexible activities are derived from published research on ‘what works’. To identify core components and flexible activities we:
1. Conduct an evidence review on a specific topic
2. Identify programs that have been shown to improve client outcomes (i.e. evidence-informed programs)
3. Review each evidence-informed program to identify core components and flexible activities that are common across them. This involves closely examining and grouping the types of activities (core components) that are undertaken as part of each program. The way these activities are implemented is also captured. These are the flexible activities within each component.
For detailed information about this process see Evidence Portal Technical Specifications.
Why does the Evidence Portal use core components?
A core components approach has been adopted for a various reasons.
A core components approach acknowledges the limitations of an evidence base of purely manualised programs. Despite the development and growing awareness of manualised programs, there are notable barriers to implementation. For example, many of these programs are copyrighted and the cost to implement them can be prohibitive.
In our work delivering important services to vulnerable children, families and communities, we often have to be flexible and responsive to changing local needs. An evidence base of purely manualised programs may inhibit such flexibility and stifle innovation. Incorporating a modular and flexible approach to service design and delivery using a core components framework offers possible advantages over traditional manualised programs. For example, manualised programs are often geared towards specific issues, but some clients will have multiple issues to address, their needs can change of time (often quite quickly and with no warning) or they may need services that do not match the length or intensity specified in a program manual (Barth et al. 2012). A core components approach acknowledges the complexity of peoples clients lives and provides service providers with an evidence-informed framework to ensure their practices are able to meet client’s needs in the best possible way.
This is not to say that manualised programs should NOT be implemented where possible. But that when a program does not fit the needs or wishes of a client, a core components approach can be used to develop a tailored and flexible combination of evidence-informed supports.
A core components approach also acknowledges the gaps that exist in the human services evidence base. Core components provide an option when there is no manualised evidence-based program known to be effective with a specific client or problem area. Many evidence-informed programs have not been evaluated in Australia, with Aboriginal and/or Torres Strait Islander communities, or culturally and linguistically diverse communities. Too often, programs that have an international evidence base are implemented in Aboriginal communities, for example, and these programs are often ineffective in that specific context. Adopting a core components approach better enables us to design and implement services that are effective, culturally safe and tailored to local community needs.
A core components approach also enables us to get evidence into practice sooner. Strengthening evidence-informed practices improves the delivery and quality of services, and in turn, client outcomes.
Where does the core components approach come from?
Our core components approach has been adapted from the literature on practice and/or common elements. The concept of distilling key activities, components, approaches and practices from manualised or evidence-informed programs was originally developed in clinical and therapeutic practice (Chorpita et al. 2005; Barth et al. 2012). It has been increasingly adopted in child and family service delivery settings, both nationally (in Victoria and South Australia for example) and internationally (see for example: Public Health England). It is a complementary method for summarizing the evidence base that builds on the work conducted to evaluate manualised programs.
The emerging evidence base highlights that the common elements approach is implementable and effective. Randomised controlled trials have demonstrated that utilising a flexible, modular practice elements approach:
- Has more sustained positive outcomes than standard treatment designs (Chorpita et al., 2013)
- Results in faster improvement on outcomes relative to usual care (Chorpita et al., 2017)
- Is more accessible and is perceived more positively by practitioners by relative to less flexible approaches (Borntrager et al. 2009; Barth et al. 2012),
- Can be delivered effectively and with fidelity by non-specialist therapists/practitioners (Bolton et al., 2014; Murray et al., 2018; Weiss et al., 2015).
In the literature, practice elements are defined as discrete clinical techniques or strategies (e.g. problem solving) used as part of a larger intervention plan (e.g. an evidence-informed program) (Chorpita et al. 2005). Practice elements are defined by their content – they may be delivered simultaneously, consecutively, used in a single session or addressed in multiple sessions.
To identify practice elements, Chorpita et al. (2005) developed a Distillation and Matching Model (DDM). This model conceptualises programs not as single units, but as combinations of individual strategies, techniques or components. The model adopts a component level of analysis with a distillation process that identifies overlapping/common components across effective programs and a matching process to client characteristics. DDM involves conducting frequency counts of the occurrence of practice elements in effective programs. It then seeks to identify any associations between practice elements and the characteristics of target groups (e.g. gender, age). For example, the model could identify that pre-school aged boy’s benefit from a similar type of program.
Over time, this model has been applied to various evidence bases and adapted as needed. See for example:
- Common elements of practice, process and implementation in out-of-school-time academic interventions for at-risk children: a systemic review (Engell et al. 2020)
- Program and practice elements for placement prevention: a review of interventions and their effectiveness in promoting home-based care (Lee et al. 2014)
- Identifying effective components of child maltreatment interventions: a meta-analysis (van der Put et al. 2018).
We too have taken this model and adapted it for our purpose of understanding and building the evidence base for child and family services. Like Chorpita et al. (2005), we develop a study data set by identifying relevant programs and extracting information about the populations they’ve been evaluated with, how they were implemented and their efficacy and effectiveness. If a program is shown to be ineffective, it is excluded from analysis. We then count frequencies to identify the most frequent components of effective programs.
Where our approaches differ is in the matching of practice elements to client characteristics. The existing evidence base for child and family services in Australia doesn’t lend itself to the kind of matching that is possible within the psychology literature (Chorpita et al. (2005) also identify gaps in the evidence as a limitation of their approach). Further, while we provide information about the target groups each flexible activity has been conducted with, we opt to provide practitioners with an evidence base of core components and flexible activities they can apply their own expertise, knowledge and skills, and the preferences and values of their clients, to determine which practice or activity should be employed.
This approach aligns with Australian literature on core components and current work being conducted by the Victorian Department of Health and Human Services (see Common Elements approach for more information) in which practitioner decision-making is at the core. Knight et al. 2018 argue that standardised core program components should be developed by using the central tenant of evidence-based practice: that is, by integrating the best available research evidence with the expertise of practitioners and service providers. Developing a service response is not simply a matter of selecting a component/element from a list of evidence-informed options. Instead, a practitioner uses their professional judgement and knowledge to consider a range of contributing factors including the client’s needs, circumstances, preferences and values and the desired outcome.
While there are many different variations for how core components, common elements, practice elements etc. are identified and implemented, the central tenants of this approach articulated in the literature include:
- A common elements or core components approach seeks to address key issues practitioners face with using an evidence base of purely manualised programs, including:
- how to differentiate between similar programs (Chorpita et al. 2005)
- how to fit a program with an individual’s specific needs and context (Chorpita et al. 2005; Knight et al. 2018; Barth et al. 2012)
- how to ensure practitioners have the required training to implement a particular program (Barth et al. 2012).
- This approach provides a structured framework for harnessing all available information and systematically organising it to enable informed decision-making in program design and implementation (Chorpita et al. 2005; Knight et al. 2018).
- Understanding the core components of evidence-informed programs that can be taught and assembled into interventions that have a more generic quality could have the advantage of broadening the availability of evidence-informed models (Lee et al. 2014). For practitioners, learning the core components, rather than a diverse collection of treatment manuals, may promote mastery and confidence in delivering effective, evidence-informed services (Chorpita et al. 2005; 2007; Barth et al. 2012).
- A core components and common elements approach prioritises client involvement and input in the supports they receive (Barth et al. 2012).
- This approach enables ‘flexibility within fidelity’; it finds a balance between ensuring programs are standardised to enable high-quality evaluations and program comparisons, but also flexible and tailored to the individual circumstances of clients and local contexts (Chorpita et al. 2005; Knight et al. 2018; Knight et al. 2017; Barth et al. 2012).
What limitations are there of the core components approach?
As with all evidence-informed approaches to service design and implementation, there are limitations to the core components approach.
A key limitation of this approach is also a limitation of the evidence base the core components are derived from. We do not know or understand the direct impact of each component or practice in isolation. While the core components are derived from the evidence on evidence-informed programs, evaluations of these programs typically evaluate programs as a whole, they don’t provide information about the effectiveness of particular practices or activities. As the core components are derived from this same literature, we too are unable to provide information about the effectiveness of a particular component. The evidence for the core components is based only on their frequency of inclusion in programs that have been found to be effective (see also Chorpita et al. 2007; 2005). The limited state of the current knowledge base limits the quality of decisions regardless of how the evidence is presented.
Last updated:

We acknowledge Aboriginal people as the First Nations Peoples of NSW and pay our respects to Elders past, present, and future.
Informed by lessons of the past, Department of Communities and Justice is improving how we work with Aboriginal people and communities. We listen and learn from the knowledge, strength and resilience of Stolen Generations Survivors, Aboriginal Elders and Aboriginal communities.
You can access our apology to the Stolen Generations.